![]()
ROTH PHILOSOPHY
R07
Early Treatment Early Treatment for Children
-
01R07
The Importance of Starting Orthodontic Treatment Early
We often hear people say, “If you start orthodontic treatment early, you can avoid having teeth extracted.” It is true that with today’s orthodontic appliances, it is possible to align all the teeth as they erupt. However, in such cases, the sole goal of treatment becomes simply aligning the teeth.
In orthodontic treatment, it is extremely important to consider the following factors, and we establish these as our treatment goals.- consideration of facial appearance
- harmony between the temporomandibular joints (TMJs) and tooth alignment
- harmony with the periodontal tissues
- functional occlusion
- aesthetic tooth alignment
What happens after the teeth are aligned is crucial. Even if all the teeth are successfully aligned, unless these treatment goals are achieved, the treatment results may not be stable, and the long-term prognosis will remain uncertain.
02R07
Cases Requiring Early Treatment
Early treatment is not necessary for every case, but prompt intervention is recommended in the following situations:
- When treatment would become difficult if delayed
- When leaving the condition untreated places a significant burden on masticatory function or the TMJs
In particular, when there is an abnormality in the positional relationship between the maxilla (upper jaw) and mandible (lower jaw), we aim to intervene during the early growth phase (around ages 6 to 9). Specific case examples will be presented to illustrate when early intervention is necessary.
-
02R07
Cases Requiring Early Treatment
Early treatment is not necessary for every case, but prompt intervention is recommended in the following situations:
- When treatment would become difficult if delayed
- When leaving the condition untreated places a significant burden on masticatory function or the TMJs
In particular, when there is an abnormality in the positional relationship between the maxilla (upper jaw) and mandible (lower jaw), we aim to intervene during the early growth phase (around ages 6 to 9). Specific case examples will be presented to illustrate when early intervention is necessary.
-
Initial



Post-splint



Final



Cephalogram
 Initial
Initial Post-splint
Post-splintCase 01R07
Mandibular Asymmetry (Lateral Deviation)
It is generally believed that this condition tends to worsen with growth. If left untreated until adulthood, the likelihood of requiring surgical intervention increases. By starting treatment before the growth spurt, we can harness the body’s natural growth to increase the likelihood of guiding the jaw structure in the desired direction. Treatment is ideally started between the ages of 6 and 9.
Initial
[7 years and 5 months]
[Face]The patient sustained a blow to the lower jaw around age 4. The mandible (lower jaw)is shifted to the left, and the chin is significantly deviated to the left.[Intraoral]The midline of the lower anterior teeth is shifted to the left. There is an anteroposterior and vertical discrepancy between the upper and lower anterior teeth, along with a slight open bite.As initial treatment, a splint was fitted to the mandible to stabilize its position and promote normal growth.
Post-splint
[After 1 year and 6 months of splint therapy]
[Face] The leftward deviation of the chin has improved and is no longer noticeable. [Intraoral] The dental midlines are now nearly aligned, and the open bite has improved.The only treatment performed was the use of a jaw-stabilization splint; no individual tooth movement was carried out. In this way, we create conditions that support normal growth. Splint wear is continued (with reduced wear time) until the start of Phase II treatment.
Final
[14 years and 10 months]
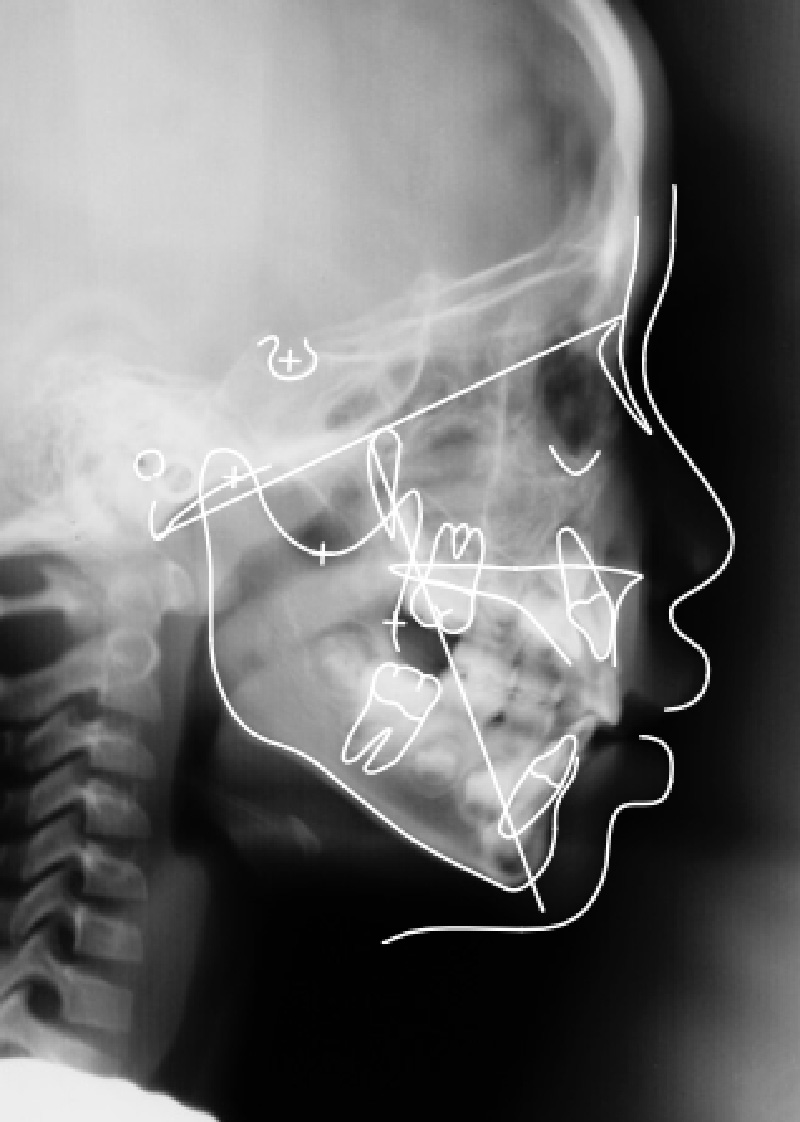
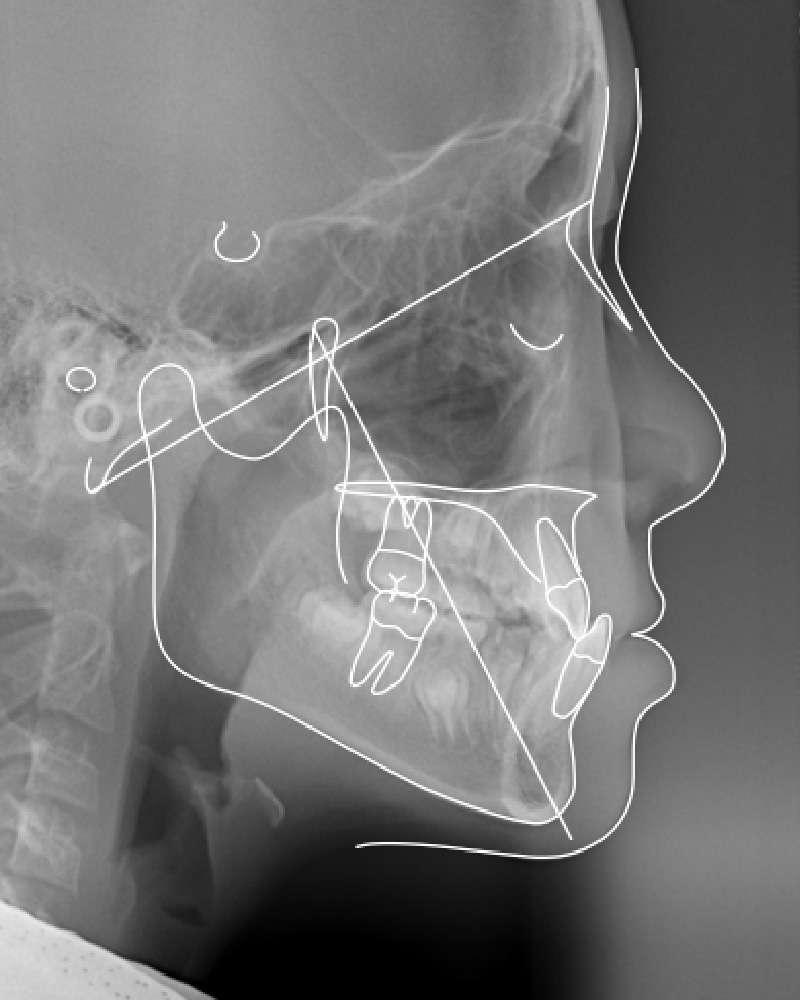
In Phase II, orthodontic treatment was performed without extractions.Cephalogram
Following splint therapy, the deviation of the chin to the left has improved. The lengths of the mandibular rami are now nearly equal on both sides.
Summary
- This approach to early treatment helps:
- effectively utilize the body’s natural growth potential
- increase the likelihood of guiding mandibular growth in a favorable direction
- prevent the condition from becoming more severe and increase the likelihood that standard orthodontic treatment will be sufficient.
-
Initial
[7 years and 5 months]
[Face]The patient sustained a blow to the lower jaw around age 4. The mandible (lower jaw)is shifted to the left, and the chin is significantly deviated to the left.[Intraoral]The midline of the lower anterior teeth is shifted to the left. There is an anteroposterior and vertical discrepancy between the upper and lower anterior teeth, along with a slight open bite.As initial treatment, a splint was fitted to the mandible to stabilize its position and promote normal growth.
-
Post-splint
[After 1 year and 6 months of splint therapy]
[Face] The leftward deviation of the chin has improved and is no longer noticeable. [Intraoral] The dental midlines are now nearly aligned, and the open bite has improved.The only treatment performed was the use of a jaw-stabilization splint; no individual tooth movement was carried out. In this way, we create conditions that support normal growth. Splint wear is continued (with reduced wear time) until the start of Phase II treatment.
-
Final
[14 years and 10 months]
In Phase II, orthodontic treatment was performed without extractions.Cephalogram
Following splint therapy, the deviation of the chin to the left has improved. The lengths of the mandibular rami are now nearly equal on both sides.
-
Cephalogram
- Initial
- Post-splint
Following splint therapy, the deviation of the chin to the left has improved. The lengths of the mandibular rami are now nearly equal on both sides.
-
Summary
- This approach to early treatment helps:
- effectively utilize the body’s natural growth potential
- increase the likelihood of guiding mandibular growth in a favorable direction
- prevent the condition from becoming more severe and increase the likelihood that standard orthodontic treatment will be sufficient.
-
Initial




R

L
Post-splint




R

L
Final



R

L
Cephalogram
 Initial
Initial Post-splint
Post-splint Final
FinalCase 02R07
Mandibular deficiency
Initial
[6 years 4 months]
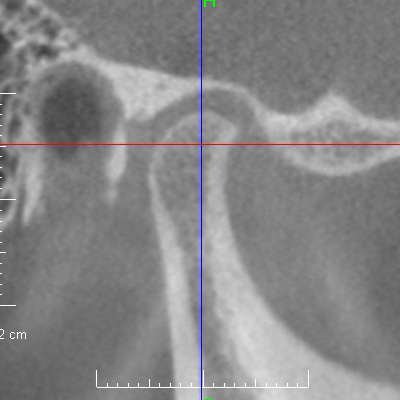
Although the patient appears normal at first glance, she had a subconscious habit of protruding the jaw forward (until the upper and lower teeth made firm contact) when biting. [TMJ CBCT Images] The condyles are significantly displaced forward from the glenoid fossae (a condition known as posturing).Since this condition deeply affects future growth, detailed examination and diagnosis—including assessment of the TMJs—are essential. In particular, MRI is necessary to assess the state of disc displacement in the TMJs. During the growth spurt, our goal is to maximize mandibular growth.
Post-splint
[After 1 year of splint therapy]
During mandibular position assessment, her true mandibular position was identified. [TMJ CBCT Images] The condyles were seated in the glenoid fossae. [Face] In this jaw position, the mandible (lower jaw) and chin were retruded. An anteroposterior gap was formed between the upper and lower anterior teeth.She continued to wear the splint (primarily at night) until transitioning to Phase II treatment involving tooth movement. Our aim was to proceed with the treatment while paying close attention until the very end to keeping the condyles seated in the glenoid fossae.
Final
[16 years and 1 month / After 2 years and 9 months of orthodontic treatment]
[Face] The mandible (lower jaw) continued to grow during treatment, and the chin moved forward significantly, resulting in a balanced facial profile. [Intraoral] The anteroposterior gap between the upper and lower anterior teeth was resolved, achieving a stable dental alignment.By utilizing the premolar extraction spaces and the growth mechanics promoting counterclockwise rotation of the mandible, we aimed for a synergistic effect with the growth spurt, resulting in further favorable mandibular growth.
Cephalogram
Although the mandible (lower jaw) was repositioned posteriorly during splint therapy, it is evident that the mandible subsequently grew significantly with counterclockwise rotation. This demonstrates how the process of stabilizing the jaw position (splint therapy) led to such substantial mandibular growth afterward.
Summary
- The TMJs were stabilized with a splint in preparation for the growth acceleration phase.
- Emphasis was placed on maximizing mandibular growth.
- Accurate diagnosis and a treatment plan with clearly defined goals are essential.
-
Initial
R
L
[6 years 4 months]
Although the patient appears normal at first glance, she had a subconscious habit of protruding the jaw forward (until the upper and lower teeth made firm contact) when biting. [TMJ CBCT Images] The condyles are significantly displaced forward from the glenoid fossae (a condition known as posturing).Since this condition deeply affects future growth, detailed examination and diagnosis—including assessment of the TMJs—are essential. In particular, MRI is necessary to assess the state of disc displacement in the TMJs. During the growth spurt, our goal is to maximize mandibular growth.
-
Post-splint
R
L
[After 1 year of splint therapy]
During mandibular position assessment, her true mandibular position was identified. [TMJ CBCT Images] The condyles were seated in the glenoid fossae. [Face] In this jaw position, the mandible (lower jaw) and chin were retruded. An anteroposterior gap was formed between the upper and lower anterior teeth.She continued to wear the splint (primarily at night) until transitioning to Phase II treatment involving tooth movement. Our aim was to proceed with the treatment while paying close attention until the very end to keeping the condyles seated in the glenoid fossae.
-
Final
R
L
[16 years and 1 month / After 2 years and 9 months of orthodontic treatment]
[Face] The mandible (lower jaw) continued to grow during treatment, and the chin moved forward significantly, resulting in a balanced facial profile. [Intraoral] The anteroposterior gap between the upper and lower anterior teeth was resolved, achieving a stable dental alignment.By utilizing the premolar extraction spaces and the growth mechanics promoting counterclockwise rotation of the mandible, we aimed for a synergistic effect with the growth spurt, resulting in further favorable mandibular growth.
-
Cephalogram
- Initial
- Post-splint
- Final
Although the mandible (lower jaw) was repositioned posteriorly during splint therapy, it is evident that the mandible subsequently grew significantly with counterclockwise rotation. This demonstrates how the process of stabilizing the jaw position (splint therapy) led to such substantial mandibular growth afterward.
-
Summary
- The TMJs were stabilized with a splint in preparation for the growth acceleration phase.
- Emphasis was placed on maximizing mandibular growth.
- Accurate diagnosis and a treatment plan with clearly defined goals are essential.
-
Initial



Final



Cephalogram
 Initial
Initial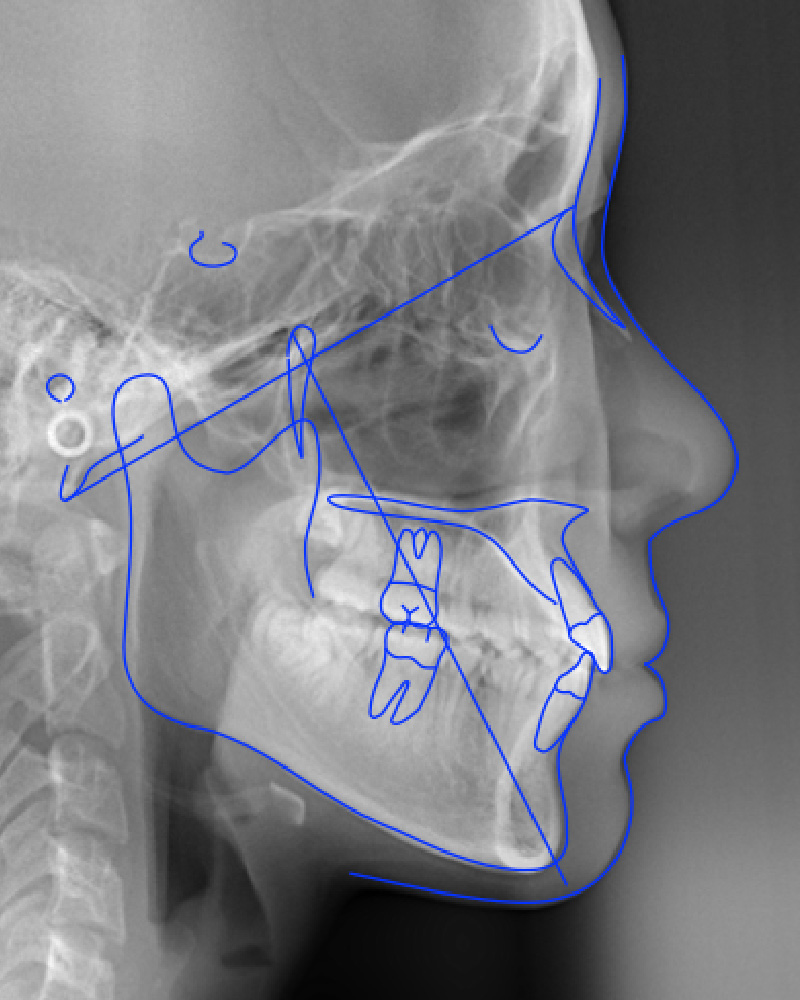 Final
FinalCase 03R07
Anterior crossbite
An anterior crossbite is a condition in which the lower teeth protrude further forward than the upper teeth (that is, the lower teeth overlap the upper teeth). This condition may result from problems with tooth positioning alone, or from discrepancies in the skeletal relationship between the maxilla (upper jaw) and mandible (lower jaw). When the problem lies in the skeletal pattern, early treatment generally facilitates correction and may have a positive impact on future growth; therefore, we recommend initiating treatment as early as possible.
Initial
[10 years and 3 months]
The patient presented to our clinic while undergoing Phase I treatment elsewhere. [Intraoral] The lower anterior teeth protruded forward, covering the upper anterior teeth. [Face] At first glance, the mandible (lower jaw) appears protruded; however, upon closer inspection, rather than the mandible being significantly protruded, the maxilla (upper jaw) appeared retruded or underdeveloped. Because the area around the ala of the nose was retruded, the mandible appeared to be protruding.The growth patterns of the maxilla and mandible differ; maxillary growth is largely complete by around age 12, while mandibular growth continues thereafter (with some variation between sexes). The window for guiding maxillary growth forward is generally between the ages of 5 and 10. In this patient, who was already 10 years and 3 months old, prompt intervention was necessary.
As an initial treatment, the maxillary sutures were loosened, followed by protraction of the maxilla. Splint therapy was performed simultaneously to correct the instability of the mandibular position while providing functional stimulation to the maxilla to promote growth. This approach stabilized the occlusion and protected the TMJs from sudden changes in the occlusion relationship. Consequently, both the occlusal relationship between the upper and lower anterior teeth and the skeletal relationship between the maxilla and mandible were improved.
Mandibular growth was monitored until growth was nearly complete. Phase II treatment was initiated at age 15 to align the teeth (treatment duration: 1 year and 7 months).
Final
The area around the ala of the nose was advanced forward, and the cheeks appeared fuller.
Cephalogram
As a result of guiding the maxilla (upper jaw) to grow forward, a significant improvement was achieved in the facial profile. Before treatment, the facial appearance resembled that of an elderly person who had lost teeth; after treatment, it transformed into a fuller and more youthful facial appearance.
Summary
The timing of orthodontic treatment varies by case, and early intervention is essential when skeletal discrepancies are present. Treating during this early period allows us to guide growth and expand treatment options.
Although attention tends to focus on the maxilla in such cases, it is equally important to monitor the mandible (lower jaw) to ensure that it grows normally. Regardless of when orthodontic treatment is performed, we first conduct comprehensive examinations and diagnoses that include the TMJs to fully understand the patient’s condition. We then provide the appropriate treatment at the optimal time—treatment that can only be performed at that specific stage—and proceed with tooth alignment in Phase II. Until then, our primary focus is on monitoring jaw growth.
One important consideration in patients with anterior crossbites is that those with a large mandible may exhibit excessive mandibular growth compared to average growth patterns; in such cases, surgical intervention may need to be considered.
-
Initial
[10 years and 3 months]
The patient presented to our clinic while undergoing Phase I treatment elsewhere. [Intraoral] The lower anterior teeth protruded forward, covering the upper anterior teeth. [Face] At first glance, the mandible (lower jaw) appears protruded; however, upon closer inspection, rather than the mandible being significantly protruded, the maxilla (upper jaw) appeared retruded or underdeveloped. Because the area around the ala of the nose was retruded, the mandible appeared to be protruding.The growth patterns of the maxilla and mandible differ; maxillary growth is largely complete by around age 12, while mandibular growth continues thereafter (with some variation between sexes). The window for guiding maxillary growth forward is generally between the ages of 5 and 10. In this patient, who was already 10 years and 3 months old, prompt intervention was necessary.
As an initial treatment, the maxillary sutures were loosened, followed by protraction of the maxilla. Splint therapy was performed simultaneously to correct the instability of the mandibular position while providing functional stimulation to the maxilla to promote growth. This approach stabilized the occlusion and protected the TMJs from sudden changes in the occlusion relationship. Consequently, both the occlusal relationship between the upper and lower anterior teeth and the skeletal relationship between the maxilla and mandible were improved.
Mandibular growth was monitored until growth was nearly complete. Phase II treatment was initiated at age 15 to align the teeth (treatment duration: 1 year and 7 months).
-
Final
The area around the ala of the nose was advanced forward, and the cheeks appeared fuller.
-
Cephalogram
- Initial
- Final
As a result of guiding the maxilla (upper jaw) to grow forward, a significant improvement was achieved in the facial profile. Before treatment, the facial appearance resembled that of an elderly person who had lost teeth; after treatment, it transformed into a fuller and more youthful facial appearance.
-
Summary
The timing of orthodontic treatment varies by case, and early intervention is essential when skeletal discrepancies are present. Treating during this early period allows us to guide growth and expand treatment options.
Although attention tends to focus on the maxilla in such cases, it is equally important to monitor the mandible (lower jaw) to ensure that it grows normally. Regardless of when orthodontic treatment is performed, we first conduct comprehensive examinations and diagnoses that include the TMJs to fully understand the patient’s condition. We then provide the appropriate treatment at the optimal time—treatment that can only be performed at that specific stage—and proceed with tooth alignment in Phase II. Until then, our primary focus is on monitoring jaw growth.
One important consideration in patients with anterior crossbites is that those with a large mandible may exhibit excessive mandibular growth compared to average growth patterns; in such cases, surgical intervention may need to be considered.
Featureof the Roth Philosophy
-
Before
After


R01
Face Design
Strong Focus on Facial Impact
When considering the principal region of the face—from the eyebrows to the chin—the tooth crowns and roots account for nearly 40% of the area. Therefore, moving the teeth has a significant impact on overall facial appearance.
-


R02
Attractive Tooth Alignment
Attractive, Beautiful Tooth Alignment
Simply straightening the teeth does not automatically result in a truly beautiful tooth alignment. A well-formed dental arch, a stable mandibular position, and healthy, stable temporomandibular joints (TMJs) contribute to a beautiful smile and promote the health of the teeth and periodontium.
-


R03
Beautiful Smile
Lips and Tooth Alignment in the Smile
The relationship between the lips and tooth alignment is surprisingly important. It can make a significant difference in the appearance of the smile.
-

R04
Stable Jaw Position
The importance of mandibular position
While the alignment of the teeth is important, it is essential to first assess the condition of the TMJs. This approach is similar to conducting a soil survey before building a house.
-

R05
Imaging
CT and MRI
In addition to cone-beam CT, which offers high accuracy with low radiation exposure, MRI is widely available in Japan and can be performed at a lower cost than in other countries. This allows us to thoroughly assess the condition of the TMJs.
-
Before
After


R06
Optimum Timing
The Right Timing for Treatment
It is important to identify the stages of a child’s growth—particularly the growth of the mandible (lower jaw)—and to tailor the treatment plan and procedures accordingly.
-
Before
After


R07
Early Treatment
Early Treatment for Children
Early treatment is recommended for cases in which treatment would become more difficult later, or in which leaving the condition untreated would place a significant burden on chewing function and the TMJs.

